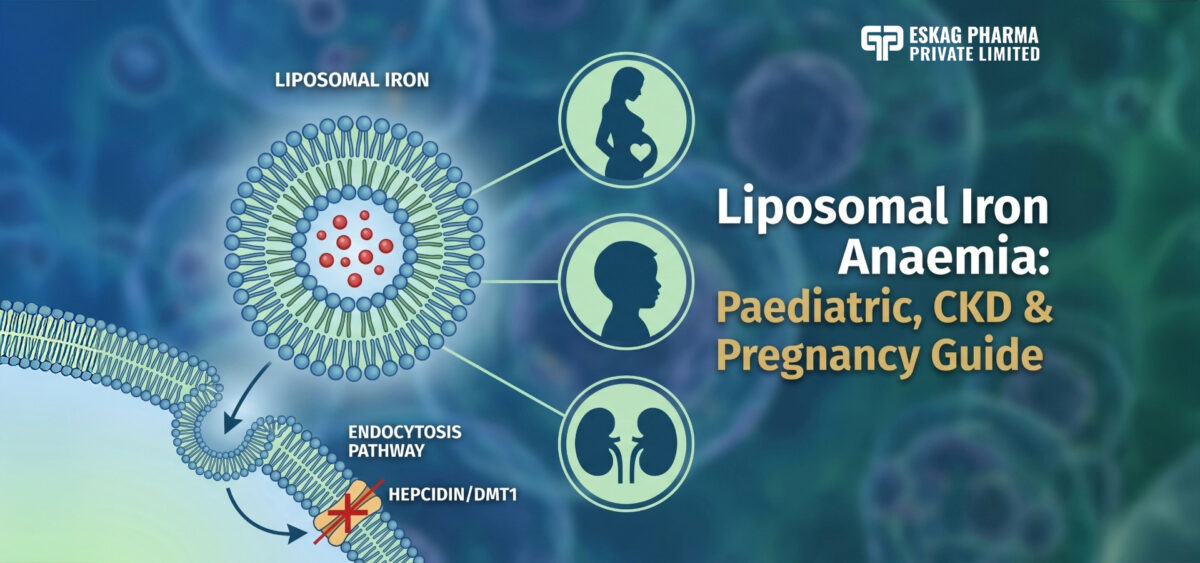
Liposomal Iron Anaemia: Paediatric, CKD & Pregnancy Guide
Iron deficiency anaemia remains the most prevalent nutritional disorder globally, yet millions of patients, children, pregnant women, and those with chronic kidney disease continue to receive a treatment their bodies cannot adequately absorb. The clinical frustration is real: a patient takes iron daily, tolerates the side effects, and still presents with subtherapeutic haemoglobin levels. This is not a compliance failure; it is a formulation failure. Liposomal iron anaemia treatment addresses this at the molecular level, bypassing hepcidin, DMT1 saturation, and dietary inhibitors entirely.
In this guide, you will find the clinical evidence and formulation considerations that matter most across paediatric, CKD, and pregnancy applications.
Key Takeaways:
- Ferrous sulfate is absorbed at only 10-15% of the ingested dose, with GI side effects occurring at an odds ratio of 2.32 compared with placebo.
- A 2025 Indian RCT confirmed liposomal iron at 1 mg/kg/day matched ferrous ascorbate at 3 mg/kg/day in children, with better GI tolerance.
- In non-dialysis CKD patients, liposomal iron achieved 96% treatment compliance, and only 12% of patients experienced GI adverse effects in a 2024 clinical trial.
Quick Answer: Liposomal iron anaemia treatment achieves 2.7x higher bioavailability than ferrous sulfate via endocytosis, bypassing hepcidin and DMT1 limits with superior GI tolerance across paediatric, CKD, and pregnancy populations.
Why Standard Iron Fails High-Risk Anaemia Patients
Liposomal iron anaemia treatment exists because conventional ferrous salts, the global standard for decades, carry a pharmacokinetic profile that actively works against the patients who need iron most.
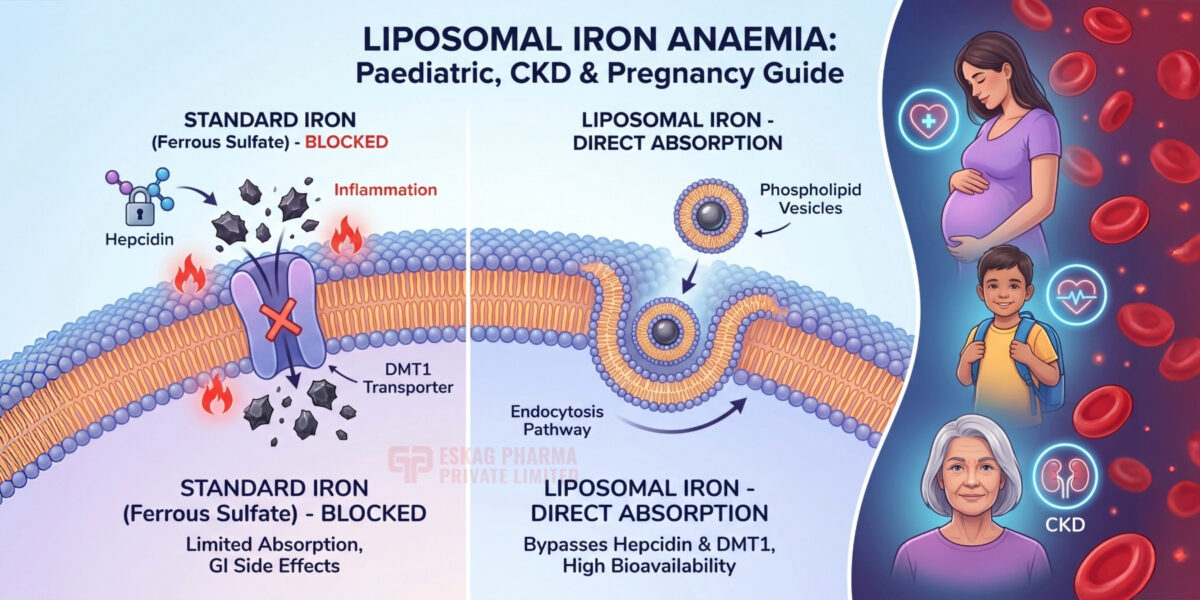
- Ferrous sulfate absorbs at only 10-15% of the ingested dose. In children, pregnant women, and CKD patients, absorption drops further due to elevated hepcidin, gut inflammation, and reduced gastric acid output.
- Ferrous sulfate increases the risk of gastrointestinal side effects, with an odds ratio of 2.32 compared with placebo; nausea, constipation, a metallic taste, and epigastric pain are expected outcomes at therapeutic doses, not rare exceptions.
- Oral iron adherence hovers at only 40-60% across clinical populations. A supplement a patient stops taking cannot correct iron deficiency, regardless of elemental iron content.
- The DMT1 transporter operates at a fixed capacity ceiling. Once saturated, additional iron increases mucosal oxidative stress without improving uptake, worsening GI irritation rather than resolving it.
- Iron is absorbed almost exclusively in the duodenum. Enteric-coated tablets release beyond the duodenum, reducing bioavailability to approximately 30% of that of the standard oral preparation.
Liposomal Iron Better Absorption: The Science Behind It
Liposomal iron anaemia treatment works where ferrous salts fail because phospholipid encapsulation replaces a broken absorption pathway with one the body already knows how to use.
How Liposomal Iron Better Absorption Bypasses DMT1
Liposomal iron’s improved absorption works through endocytosis, the same pathway cells use to internalise nutrients directly across the intestinal membrane. The phospholipid bilayer fuses with enterocytes, delivering ferric pyrophosphate into circulation without requiring DMT1 transport or gastric acid activation.
Why Iron Deficiency Anaemia Persists with Standard Oral Iron
Iron deficiency anaemia persists in high-risk populations because hepcidin — the iron-regulatory hormone- actively suppresses DMT1 expression during inflammation, infection, and CKD anaemia management scenarios. This means the very conditions that create iron deficiency simultaneously block conventional oral iron from being absorbed, creating a clinical deadlock that dose escalation cannot resolve.
Liposomal Iron Anaemia Outcomes: Bioavailability vs Ferrous Salts
Liposomal iron anaemia formulations achieve 2.7-fold higher bioavailability than ferrous sulfate, as confirmed by encapsulation efficiency exceeding 89% in pharmaceutical-grade production. For paediatric anaemia treatment and CKD anaemia management, this bioavailability advantage allows clinically effective doses at a fraction of the elemental iron required by ferrous salts, directly reducing the GI burden that drives non-compliance.
Liposomal Iron Anaemia in Paediatric Patients
Children represent the most clinically urgent population for liposomal iron anaemia intervention; standard iron fails them on all three fronts: tolerability, compliance, and developmental timing.
Pediatric Anaemia Treatment: Why Standard Iron Fails Children
Pediatric anaemia treatment with conventional ferrous salts faces three compounding problems unique to children. First, therapeutic doses cause taste aversion and GI distress that parents frequently discontinue before haemoglobin recovers. Second, children metabolise iron differently; their absorptive capacity varies significantly with age, growth phase, and inflammatory status. Third, the consequence of under-treatment in early childhood is not just anaemia; it is irreversible developmental loss during a window that cannot be reopened.
Liposomal Iron Anaemia RCT Evidence in Children
A 2025 randomised controlled trial directly compared liposomal iron with ferrous ascorbate in 98 children aged 6–60 months with confirmed iron-deficiency anaemia [1]. The liposomal group received 1 mg/kg/day; the ferrous ascorbate group received 3 mg/kg/day. Both groups achieved equivalent haemoglobin improvement over one month, but the liposomal group reached that outcome at one-third the elemental iron dose, with significantly better GI tolerability and higher completion rates.
Iron Deficiency Anaemia and Cognitive Risk in Paediatric Patients
Iron deficiency anaemia in children under five does not present as fatigue alone; it impairs myelination, dopamine synthesis, and hippocampal development during the period of fastest brain growth. These neurological effects persist beyond haemoglobin correction; children treated late show measurable cognitive and behavioural deficits even after iron stores normalise. A formulation that children actually complete, because it causes no metallic taste or GI pain, is not a convenience feature. It is a clinical necessity.
CKD Anaemia Management with Liposomal Iron
CKD anaemia management demands a different clinical logic: the same inflammation that damages the kidneys also triggers hepcidin overproduction, which shuts down the absorption pathway that conventional oral iron relies on entirely.
CKD Anaemia Management: Why Hepcidin Blocks Oral Iron
Hepcidin is the liver-produced hormone that regulates systemic iron availability. In CKD, chronic inflammation and reduced renal clearance cause hepcidin to accumulate at abnormally high levels. Elevated hepcidin degrades ferroportin, the only export channel through which intestinal iron enters circulation. Conventional oral iron reaches the duodenal wall and stops there. The absorption gate is closed at the molecular level, and no increase in the oral dose can override it.
Liposomal Iron Better Absorption in Non-Dialysis CKD Patients
Liposomal iron better absorption in CKD works because endocytosis does not depend on ferroportin. The phospholipid vesicle fuses directly with enterocyte membranes and transfers iron into the lymphatic system, a route hepcidin cannot regulate. This makes liposomal iron the only oral formulation that retains a functional absorption pathway in the inflammatory environment characteristic of CKD stages G3 and G4, where hepcidin elevation is significant but IV iron is not yet clinically warranted.
Liposomal Iron Anaemia Evidence: CKD Clinical Trial Data
A 2024 prospective study by Cesarano et al., published in Nutrients, evaluated oral liposomal iron supplementation in non-dialysis CKD patients with confirmed iron deficiency. The results were clinically notable: GI adverse effects occurred in only 12% of patients, and treatment compliance reached 96%, a figure that conventional oral iron studies have never approached in this population [2]. For haemodialysis patients, KDIGO 2026 still recommends IV iron as first-line; liposomal oral iron is most appropriate for non-dialysis and peritoneal dialysis stages, where absorption remains partially intact.
Liposomal Iron Formulation Manufacturer: Sourcing Guide
Not every manufacturer that lists liposomal iron can validate encapsulation efficiency, confirm the purity of ferric pyrophosphate by HPLC, or provide the stability dossiers required by FSSAI and export regulators. The gap between a generic iron capsule and a pharmaceutical-grade liposomal iron formulation is significant, and it shows in clinical outcomes. Eskag Pharma Private Limited bridges that gap. With five decades of WHO-GMP-certified manufacturing from its SIDCUL, Haridwar facility, an existing validated liposomal iron tablet formulation, active export partnerships across 50+ countries, and end-to-end regulatory documentation, Eskag Pharma provides what most contract manufacturers cannot: a production-ready liposomal iron product backed by verifiable quality systems.
Final Thoughts
Liposomal iron anaemia treatment is a clinical response to a well-documented failure: standard oral iron has never fully resolved anaemia in vulnerable populations. If you are a formulation buyer, the first question to ask your manufacturer is not price; it is whether they can provide encapsulation efficiency data and HPLC-verified potency of ferric pyrophosphate per batch. For paediatric applications, confirm the formulation is liquid-compatible and taste-neutral. For CKD, verify that the cited clinical evidence is from non-dialysis populations. The brands that hold durable market positions in specialised iron supplementation are those whose claims rest on verifiable batch data.
References
- Rangaraj S, Suresh P, Sundar S, Raju P. Liposomal Iron vs. Conventional Iron in the Treatment of Iron Deficiency Anemia in Children: A Randomized Controlled Trial. Cureus. 2025 Nov 18;17(11):e97183. doi: 10.7759/cureus.97183. PMID: 41431535; PMCID: PMC12718472.
- Cesarano D, Borrelli S, Campilongo G, D’Ambra A, Papadia F, Garofalo C, De Marco A, Marzano F, Ruotolo C, Gesualdo L, Cirillo P, Minutolo R. Efficacy and Safety of Oral Supplementation with Liposomal Iron in Non-Dialysis Chronic Kidney Disease Patients with Iron Deficiency. Nutrients. 2024 Apr 24;16(9):1255. doi: 10.3390/nu16091255. PMID: 38732502; PMCID: PMC11085822.
-
 📅 June 27, 2026
📅 June 27, 2026
The global nutraceutical industry faces a critical... -
 📅 June 27, 2026
📅 June 27, 2026
Iron deficiency anaemia remains the most prevalent... -
 📅 June 26, 2026
📅 June 26, 2026
Uneven skin tone, persistent redness, and acne tha... -
 📅 June 26, 2026
📅 June 26, 2026
If you struggle to switch off after a long day, yo... -
 📅 June 26, 2026
📅 June 26, 2026
India’s sleep aid market is on course to rea... -
 📅 June 26, 2026
📅 June 26, 2026
Key Takeaways The First-Pass Barrier: Traditional ... -
 📅 June 24, 2026
📅 June 24, 2026
Sleep disruption is not simply a lifestyle inconve... -
 📅 June 18, 2026
📅 June 18, 2026
The sleep supplement industry is undergoing a fund... -
 📅 May 28, 2026
📅 May 28, 2026
Anaemia is one of the most common and consequentia... -
 📅 May 27, 2026
📅 May 27, 2026
Patients struggling with iron deficiency anaemia o...
Ferrous sulfate is absorbed at only 10–15% of the ingested dose and causes GI side effects in most patients. Liposomal iron bypasses DMT1 via endocytosis, achieves 2.7x higher bioavailability, and causes no reactive oxygen species damage to the gut lining.
Yes. A 2025 Indian RCT confirmed liposomal iron at 1 mg/kg/day matched ferrous ascorbate at 3 mg/kg/day in children aged 6–60 months, at one-third the elemental dose, with better GI tolerability and completion rates.
In non-dialysis CKD stages G3–G4, yes. Confirmed 96% compliance and only 12% GI side effects. For haemodialysis patients, KDIGO 2026 still recommends IV iron as first-line; liposomal oral iron does not replace it in dialysis-dependent patients.
HPLC-verified ferric pyrophosphate potency, encapsulation efficiency above 85%, particle size distribution per batch, 24-month accelerated stability data, and NABL-accredited third-party testing certificates. Any manufacturer unable to supply these per batch is not production-ready for clinical-grade liposomal iron.
Dry-form liposomal iron achieves 24-30 months of stability at ambient conditions with nitrogen-flush processing and tocopherol co-formulation. Shelf-life claim must be confirmed by PDI stability and potency retention data for each batch, not by physical appearance alone.